- Small Penis Treatment Dubai
- Longevity Health Check Dubai
- Male Genital Cosmetology Dubai
- Male Sexual Problems Treatment Dubai
- Prevention Health Check Dubai
- Premature Ejaculation Treatment in Dubai
- Erectile Dysfunction Treatment in Dubai
- Azoospermia (Zero Sperm Count) Treatment in Dubai
- Peyronie’s Disease Treatment in Dubai
- Reduced Penile Girth Treatment in Dubai
Peyronie’s Disease Treatment in Dubai i
Minimally Invasive Collagenase Therapy, Regenerative Support & Erectile Function Optimization (DHA-Compliant)
This document provides a scientifically structured, regulatory-conscious overview of Peyronie’s disease management with emphasis on minimally invasive collagenase therapy integrated with regenerative strategies and erectile function assessment. All treatments are delivered under licensed medical supervision. Clinical outcomes vary and no guarantees are provided.
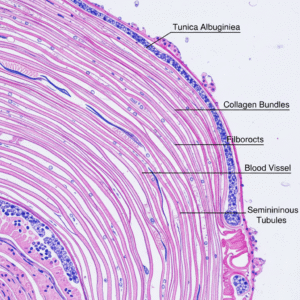
Penile Anatomy & Plaque Formation (Illustration Section)
Tunica albuginea cross-sectional anatomy
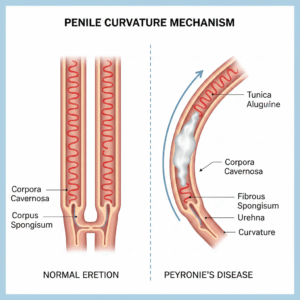
Penile curvature mechanism diagram
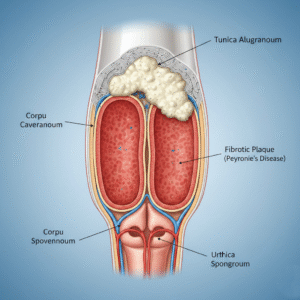
Fibrotic plaque within tunica albuginea illustration
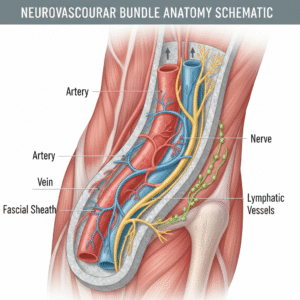
Neurovascular bundle anatomy schematic
Peyronie’s disease involves fibrotic plaque formation within the tunica albuginea. This disrupts normal tissue elasticity and causes asymmetric expansion during erection, resulting in curvature.
Clinical Overview of Peyronie’s Disease
Peyronie’s disease is an acquired connective tissue disorder characterized by excessive collagen deposition within the tunica albuginea. It often progresses through:
- Acute inflammatory phase (pain, evolving curvature)
- Chronic stable phase (persistent curvature, reduced pain)
Plaque formation may lead to penile shortening, indentation, hinge deformity, and erectile dysfunction.
Associated Erectile Dysfunction (ED)
Erectile dysfunction frequently coexists with Peyronie’s disease due to:
- Veno-occlusive dysfunction
- Impaired cavernosal expansion
- Endothelial dysfunction
- Psychogenic distress
A comprehensive erectile assessment is essential prior to treatment planning. Management may include vascular optimization, regenerative support, or pharmacologic therapy when indicated.
Minimally Invasive Collagenase Therapy (Primary Modality)
Collagenase is an enzyme that selectively degrades type I and III collagen within Peyronie’s plaques.
Key Features:
- Ultrasound-guided intralesional injection
- Targeted enzymatic softening of fibrotic plaque
- Gradual curvature reduction
- Minimally invasive approach
Multiple treatment cycles may be required depending on plaque characteristics and curvature severity.
Collagenase therapy aims to remodel plaque while preserving surrounding healthy tissue, making it preferable to excisional surgery in many mild-to-moderate cases.
Surgical Considerations: Limited Role of Excision
Traditional plaque excision involves removal of fibrotic tissue and graft placement. While effective in severe deformity, excisional surgery carries risks including:
- Erectile dysfunction
- Sensory changes
- Penile shortening
- Longer recovery period
Modern practice favors minimally invasive enzymatic therapy first. Incision and grafting (without full excision) may be considered in selected severe or refractory cases. Excision-based approaches are reserved for complex deformities where conservative therapy fails.
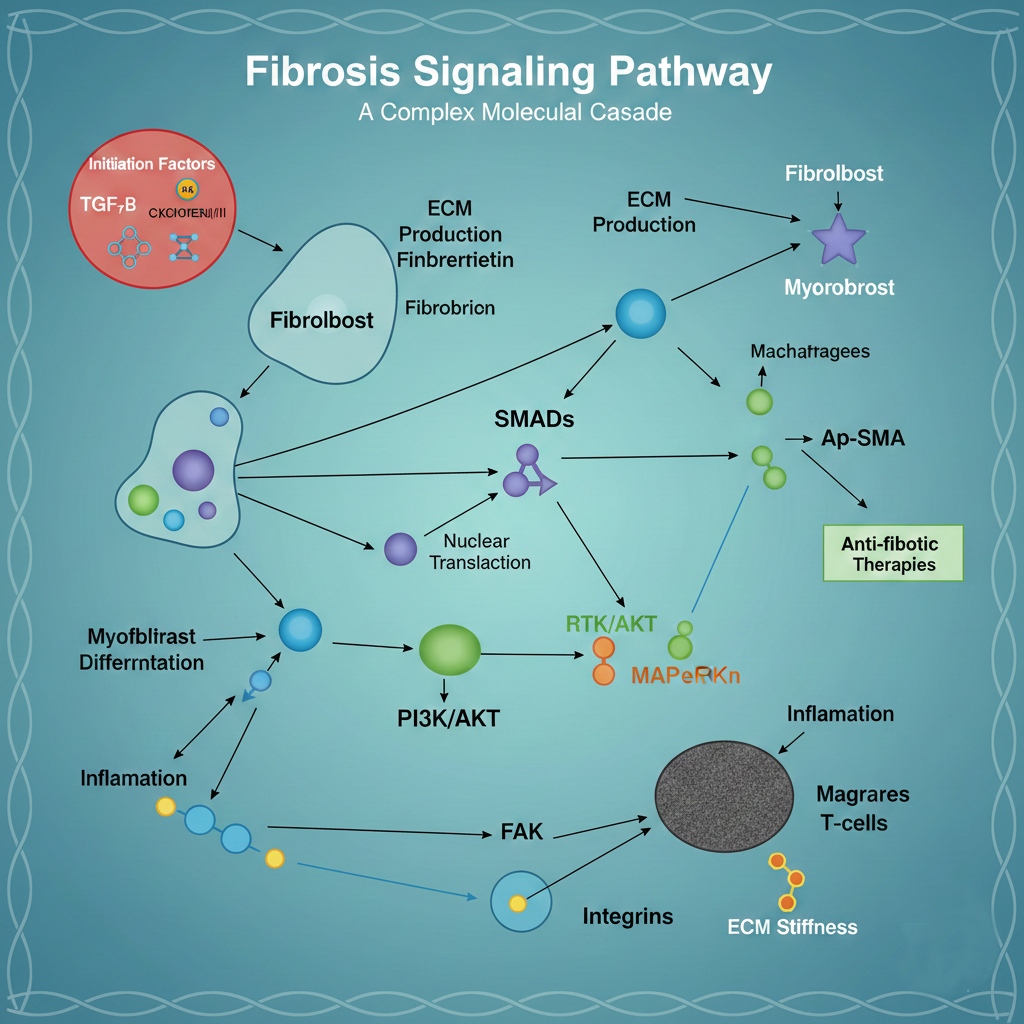
Cellular Rejuvenation & Exosome-Based Support
Fibrosis signaling pathway diagram
Exosome-mediated tissue signaling illustration
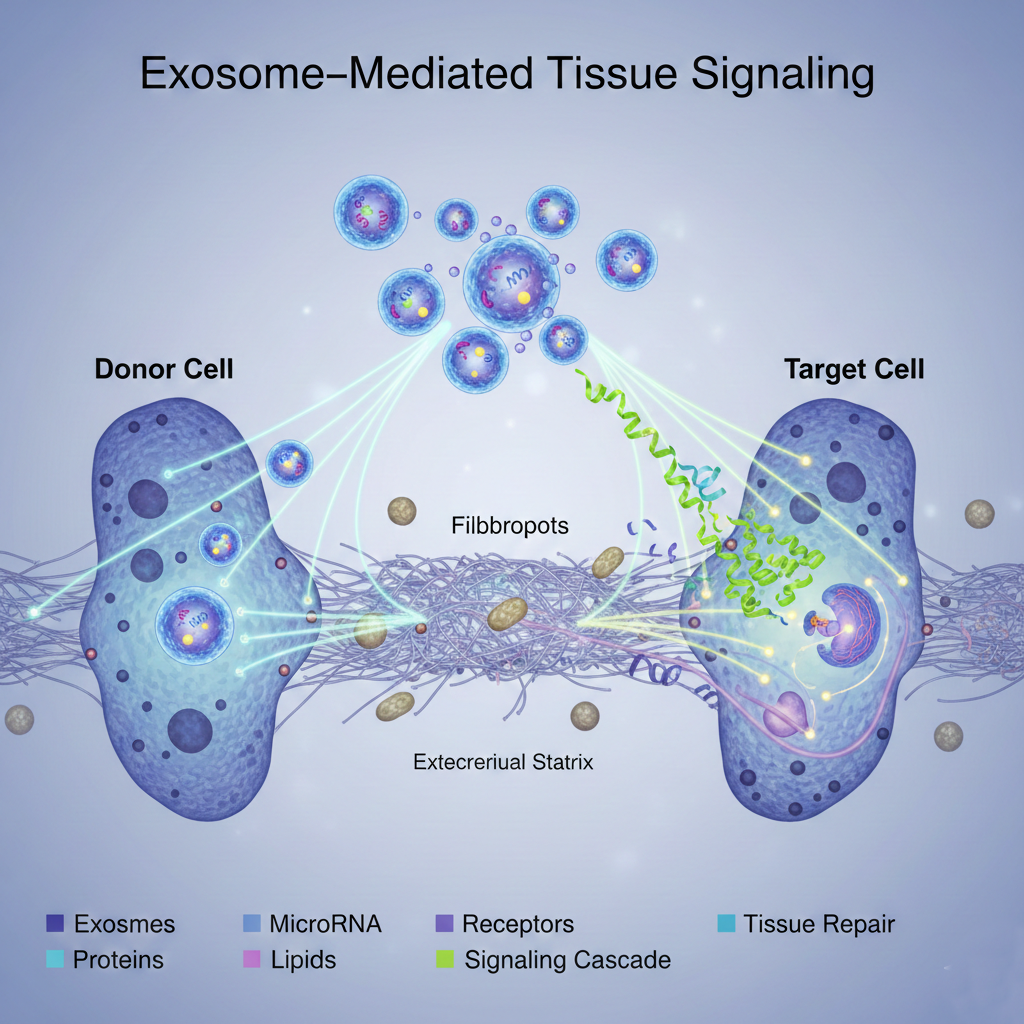
Regenerative therapy aims to modulate the biological drivers of fibrosis and inflammation.
Proposed mechanisms include:
- Downregulation of pro-fibrotic signaling (e.g., TGF-beta pathways)
- Reduction of chronic inflammatory mediators
- Enhancement of microvascular perfusion
- Support of extracellular matrix remodeling
This approach complements collagenase by supporting healthier tissue recovery.
Integrated Treatment Strategy
In selected patients, treatment may include:
- Intralesional collagenase cycles
- Local regenerative therapy
- Systemic exosome support in inflammatory/metabolic cases
- Erectile dysfunction optimization
Protocols are individualized based on disease stage, curvature degree, and erectile status.
Integrated Treatment Strategy
Additional supportive therapies may include
- Low-Intensity Shockwave Therapy for vascular support
- Platelet-derived growth factor therapy in selected cases
- Penile traction therapy under supervision
Selection depends on clinical findings and medical necessity.
Expected Outcomes
Some patients may experience:
- Reduction in curvature
- Decreased plaque firmness
- Improved erectile quality
- Enhanced sexual confidence
Response depends on plaque characteristics, disease phase, and vascular health. No outcome can be guaranteed.
Frequently Asked Questions
1.Is collagenase better than surgery?
For many mild-to-moderate cases, collagenase offers a minimally invasive alternative with lower risk compared to excision-based surgery.
2.When is surgery necessary?
Incision and grafting may be considered in severe deformity or when minimally invasive therapies are ineffective.
3.Can Peyronie’s cause erectile dysfunction?
Yes. Erectile dysfunction is common and should be evaluated and treated as part of comprehensive care.
4.Is regenerative therapy experimental?
Regenerative approaches are evolving and should be discussed thoroughly during consultation.
5.How many collagenase cycles are required?
Multiple cycles may be necessary depending on plaque response and curvature severity.
6.Is treatment painful?
Procedures are minimally invasive and generally well tolerated under appropriate medical supervision.

Self-Assessment Questionnaire for Premature Ejaculation
Instructions: This self-assessment is intended for personal screening purposes only and does not replace a medical consultation. Answer each question honestly based on your experience over the past 6 months.
This questionnaire is a screening tool only and is not diagnostic. Information provided here is for educational purposes.