- Genital Growth Concerns
- Health Longevity Check
- Male Genital Cosmetology
- Male Sexual Problems
- Prevention Health Check
- Premature Ejaculation Treatment in Dubai
- Erectile Dysfunction Treatment in Dubai
- Azoospermia (Zero Sperm Count) Treatment in Dubai
- Peyronie’s Disease Treatment in Dubai
- Reduced Penile Girth Treatment in Dubai
Azoospermia (Zero Sperm Count) Treatment in Dubai
Comprehensive Regenerative Framework Including Autologous Mesenchymal-Derived Cellular Therapy, Exosomes & Hormonal Optimization
This document provides a detailed, scientifically structured and regulatory-conscious overview of advanced regenerative approaches for azoospermia. All therapies discussed are performed under licensed medical supervision with informed consent. Clinical response varies and no outcomes can be guaranteed.
Clinical Overview of Azoospermia
Azoospermia is defined as the absence of sperm in at least two properly conducted semen analyses. It is classified into:
Obstructive Azoospermia (OA): Normal spermatogenesis with physical blockage preventing sperm release.
Non‑Obstructive Azoospermia (NOA): Impaired or absent sperm production due to intrinsic testicular dysfunction.
NOA is often associated with endocrine imbalance, oxidative stress, inflammation, genetic factors, microvascular compromise, metabolic disease, or age‑related degeneration.

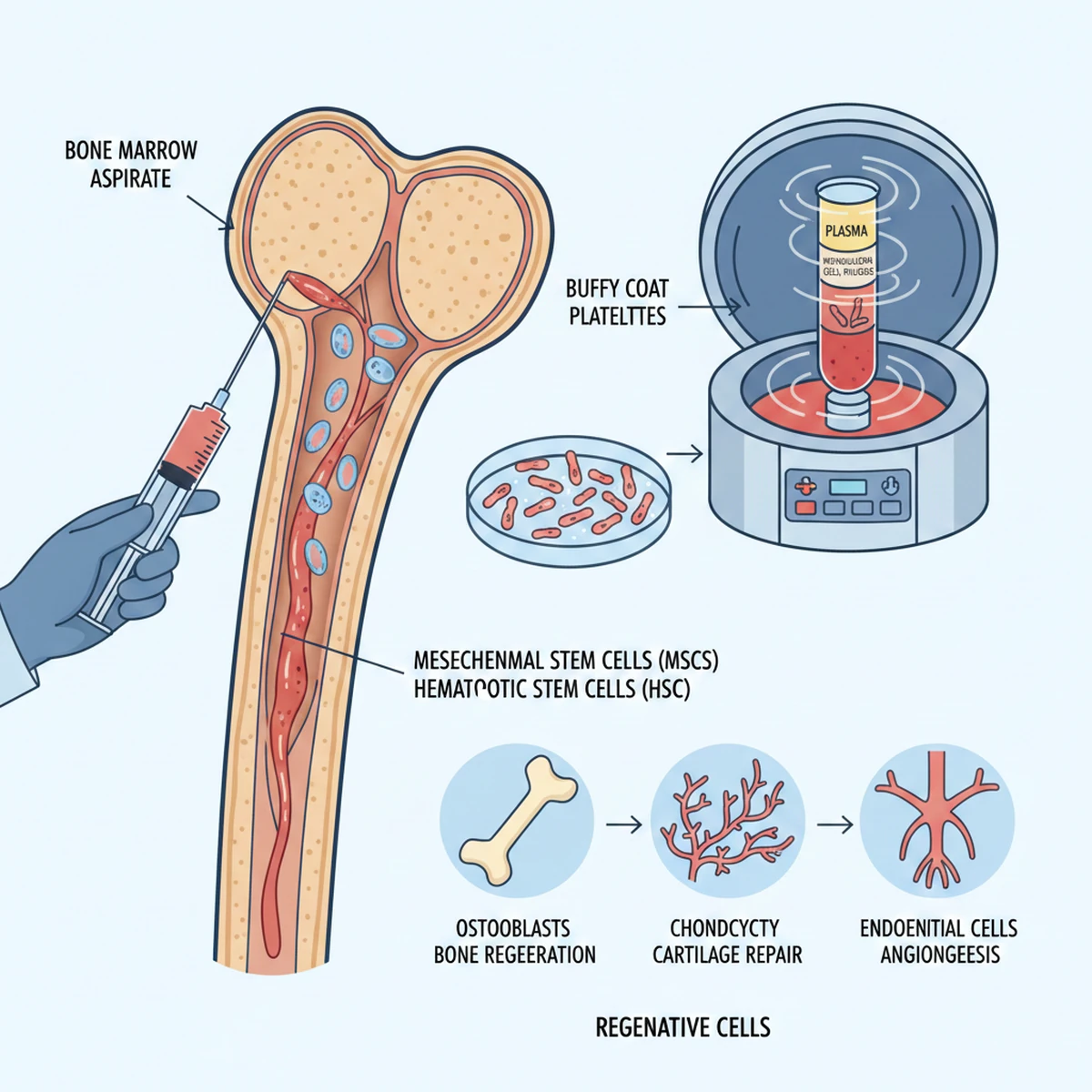
Autologous Mesenchymal-Derived Regenerative Cellular Therapy (MDRC)
For clarity and patient communication, the term ‘mesenchymal-derived regenerative cells (MDRCs)’ is used to describe autologous connective-tissue-origin cellular preparations.
Bone marrow aspirate–derived regenerative cells
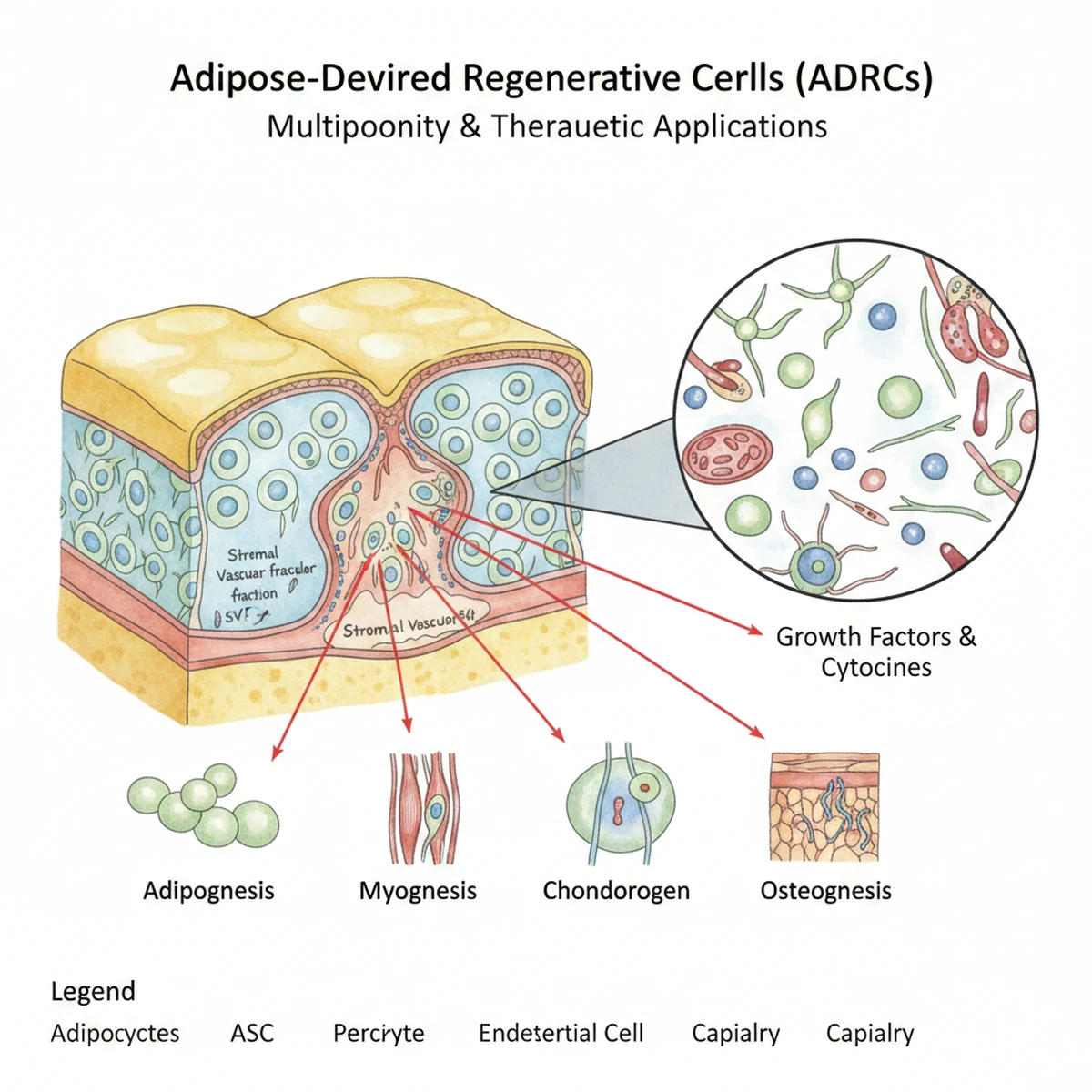
Adipose (fat)-derived regenerative cells
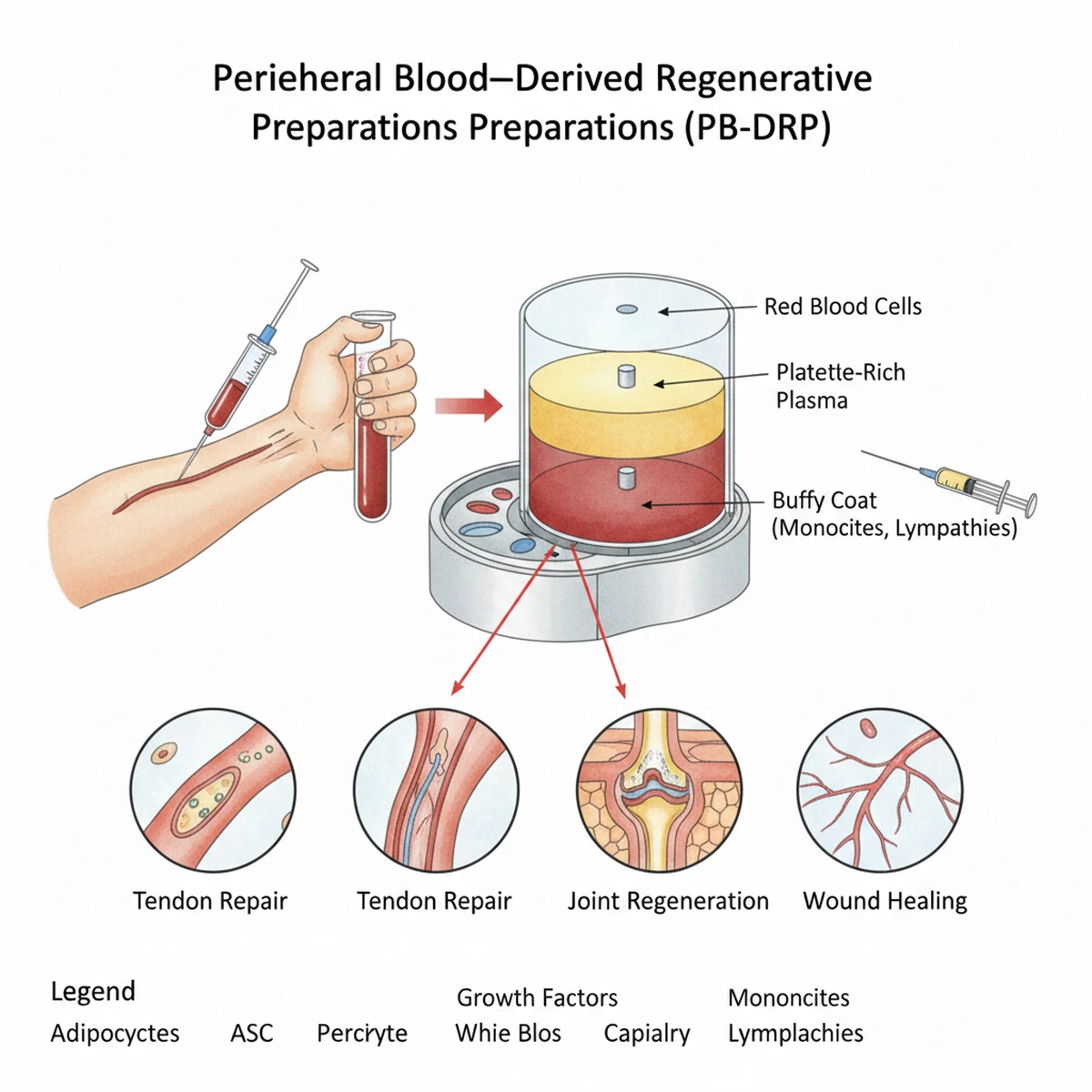
Peripheral blood–derived regenerative preparations
Autologous sourcing minimizes immunologic risk and disease transmission.
Biological Rationale:
MDRCs exert effects primarily via paracrine signaling. They release growth factors, cytokines, and extracellular vesicles that may:
- Support seminiferous tubule microenvironment
- Enhance Sertoli and Leydig cell signaling
- Promote angiogenic pathways
- Modulate inflammatory cytokines
- Improve oxidative stress balance
- Support microvascular perfusion

Intratesticular (Localized) Administration
Ultrasound-guided intratesticular delivery allows targeted placement of regenerative material into testicular parenchyma.
Key considerations:
- Performed under sterile conditions with local anesthesia.
- May require 1–3 sessions depending on biological response.
- Sessions are typically spaced weeks to months apart.
- Monitoring includes semen analysis and hormonal evaluation.
Potential Risks:
- Temporary discomfort
- Minor hematoma
- Infection (rare)
- Limited long-term data in large populations
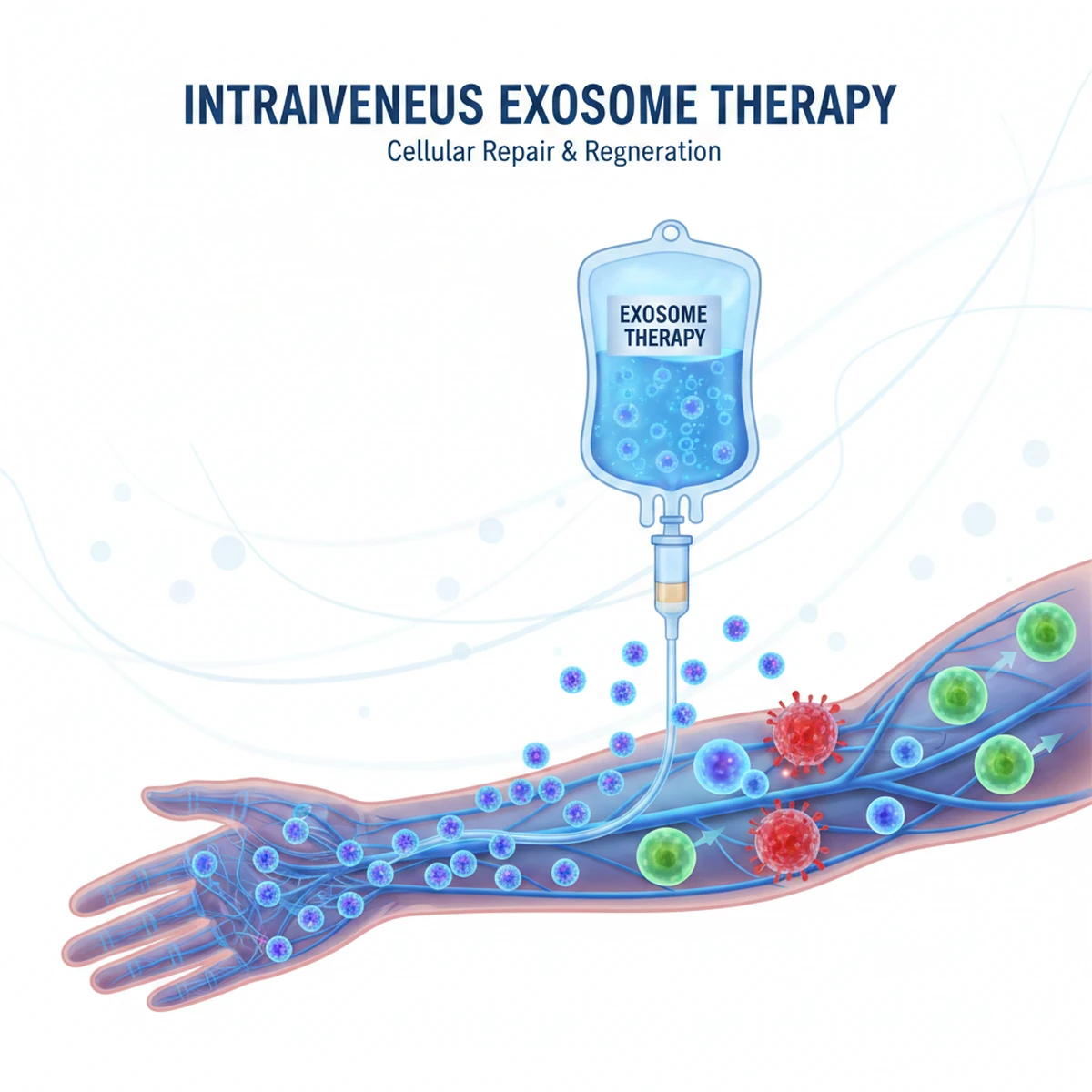
Intravenous Exosome Therapy
Exosomes are extracellular vesicles involved in cellular communication. Intravenous administration aims to support systemic endothelial health, reduce inflammatory burden, and improve vascular microcirculation.
In fertility-focused protocols, IV exosomes may:
- Support systemic anti-inflammatory signaling
- Enhance endothelial nitric oxide pathways
- Improve metabolic-inflammatory balance
- Complement localized regenerative therapy
Combination Protocol Strategy
In selected patients, a staged combination approach may include:
- Intratesticular MDRC therapy (1–3 sessions)
- Intermittent IV exosome therapy
- Concurrent hormonal optimization
This integrated strategy aims to support both local testicular microenvironment and systemic vascular/endocrine contributors.
Hormonal Optimization
Hormonal correction remains essential in patients with endocrine abnormalities.
Evidence-based options include:
- Gonadotropin therapy (hCG ± hMG) for hypogonadotropic hypogonadism
- Selective estrogen receptor modulators (e.g., clomiphene citrate)
- Aromatase inhibitors when T/E2 imbalance is present
Hormonal optimization may improve spermatogenic signaling and may be used alongside regenerative approaches.
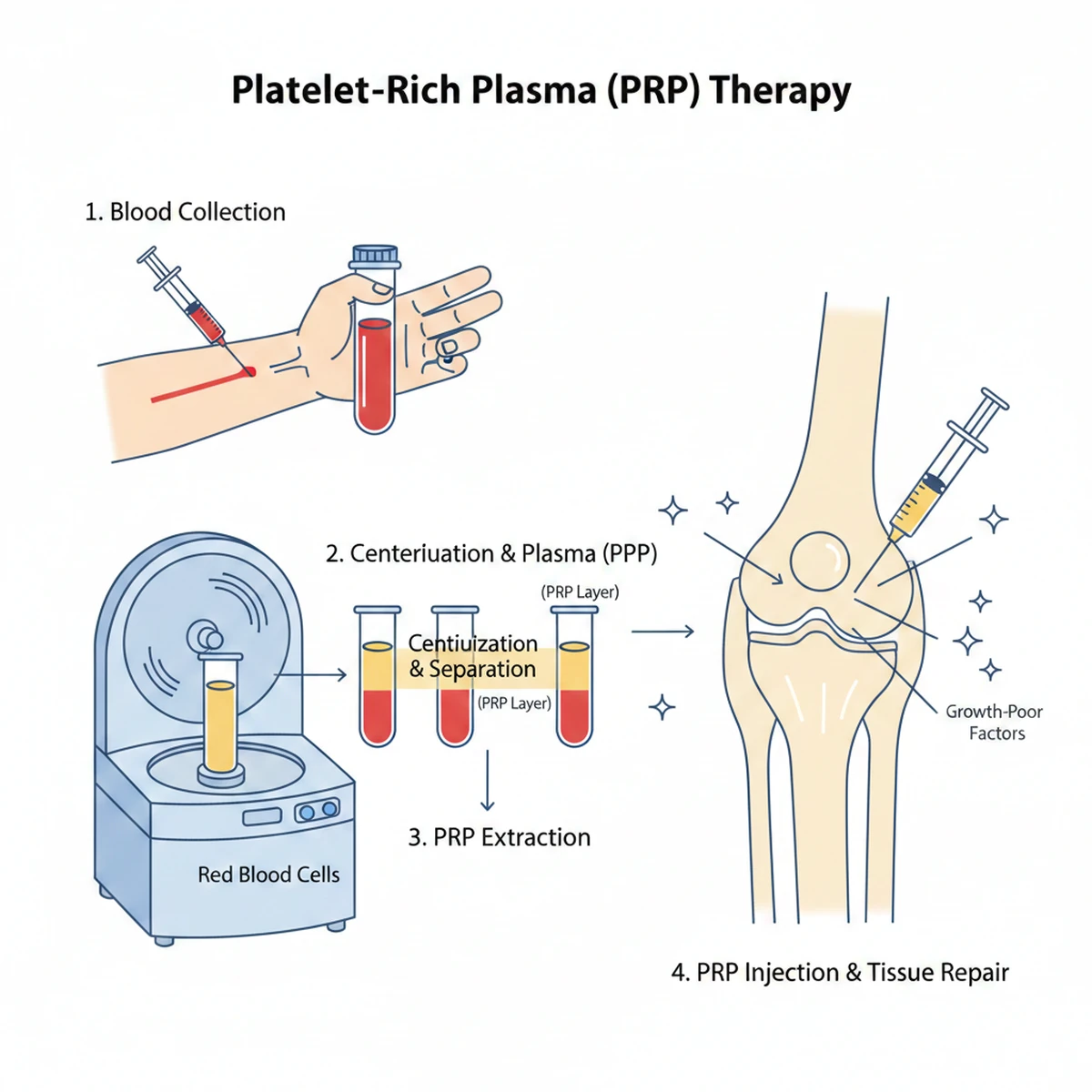
Intratesticular PRP – Evidence Review
Platelet-Rich Plasma (PRP) delivers concentrated autologous growth factors.
Current Evidence Summary:
- Small human studies report variable improvements in sperm retrieval rates.
- Animal models demonstrate possible microenvironment improvement.
- Evidence remains limited by small sample sizes and lack of large randomized trials.
Conclusion:
PRP may be considered investigational. Outcomes are inconsistent, and it should not be considered uniformly effective.
Expected Outcomes & Timeline
Spermatogenesis cycle duration is approximately 74 days.
Biological response, if observed, may require several months.
Improvement depends on baseline pathology, genetic factors, metabolic health, and endocrine balance.
No outcome can be guaranteed.

Frequently Asked Questions
Is autologous regenerative cellular therapy safe?
Early human studies suggest acceptable short-term safety when performed by experienced physicians. Long-term data are limited.
.How many intratesticular sessions are required?
Protocols often involve 1–3 sessions depending on clinical response.
Is IV exosome therapy experimental?
Yes. It is considered investigational in fertility applications.
Is PRP into the test reliable?
Evidence is mixed. It may benefit selected patients but is not consistently effective.
Can hormonal therapy be combined?
Yes. Hormonal optimization is essential when endocrine abnormalities are present.

Self-Assessment Questionnaire for Erectile Dysfunction
Instructions: This self-assessment is intended for personal screening purposes only and does not replace a medical consultation. Answer each question honestly based on your experience over the past 6 months.
This questionnaire is a screening tool only and is not diagnostic. Information provided here is for educational purposes.