- Small Penis Treatment Dubai
- Longevity Health Check Dubai
- Male Genital Cosmetology Dubai
- Male Sexual Problems Treatment Dubai
- Prevention Health Check Dubai
- Premature Ejaculation Treatment in Dubai
- Erectile Dysfunction Treatment in Dubai
- Azoospermia (Zero Sperm Count) Treatment in Dubai
- Peyronie’s Disease Treatment in Dubai
- Reduced Penile Girth Treatment in Dubai
Erectile Dysfunction Treatment in Dubai
Advanced Regenerative & Exosome-Based Clinical Framework (DHA-Compliant)
This document outlines a scientifically structured, regulatory-conscious overview of erectile dysfunction (ED) management using advanced cellular regenerative therapies and exosome-based strategies. All interventions are delivered under licensed medical supervision in accordance with UAE healthcare regulations. Clinical outcomes vary between individuals, and no guarantees are provided.
Penile Anatomy & Erectile Physiology (Illustration Section)
- Corpora cavernosa cross-sectional anatomy
- Penile arterial inflow and venous occlusion mechanism
- Nitric oxide (NO) signaling pathway diagram
- Endothelial function schematic
Erection is a neurovascular process involving coordinated arterial inflow, smooth muscle relaxation, veno-occlusive function, and intact neural signaling. Disruption at any level may result in erectile dysfunction.


Understanding Erectile Dysfunction: Clinical Mechanisms
Erectile dysfunction is defined as the persistent inability to achieve or maintain an erection sufficient for satisfactory sexual performance. ED is commonly multifactorial and may involve:
- Endothelial dysfunction and impaired nitric oxide signaling
- Reduced arterial inflow or microvascular disease
- Venous leakage
- Peripheral neuropathy
- Post-surgical neurovascular injury
- Diabetes-related vascular compromise
- Age-associated tissue degeneration
- Chronic inflammation
Cellular Regenerative Therapy: Scientific Rationale
Advanced mesenchymal-derived cellular therapy (connective tissue–origin regenerative cells) is studied for its role in tissue repair, angiogenic signaling, and neurovascular support. These biologically active cellular components are investigated for their capacity to enhance endothelial recovery, modulate inflammation, and support tissue remodeling.
Proposed biological mechanisms include:
- Paracrine signaling to enhance angiogenesis
- Support of endothelial nitric oxide synthase (eNOS) pathways
- Modulation of inflammatory cytokines
- Promotion of extracellular matrix stabilization
- Support of peripheral nerve microenvironment repair

Intracavernosal Cellular Regenerative Therapy
Intracavernosal injection anatomical guidance diagram
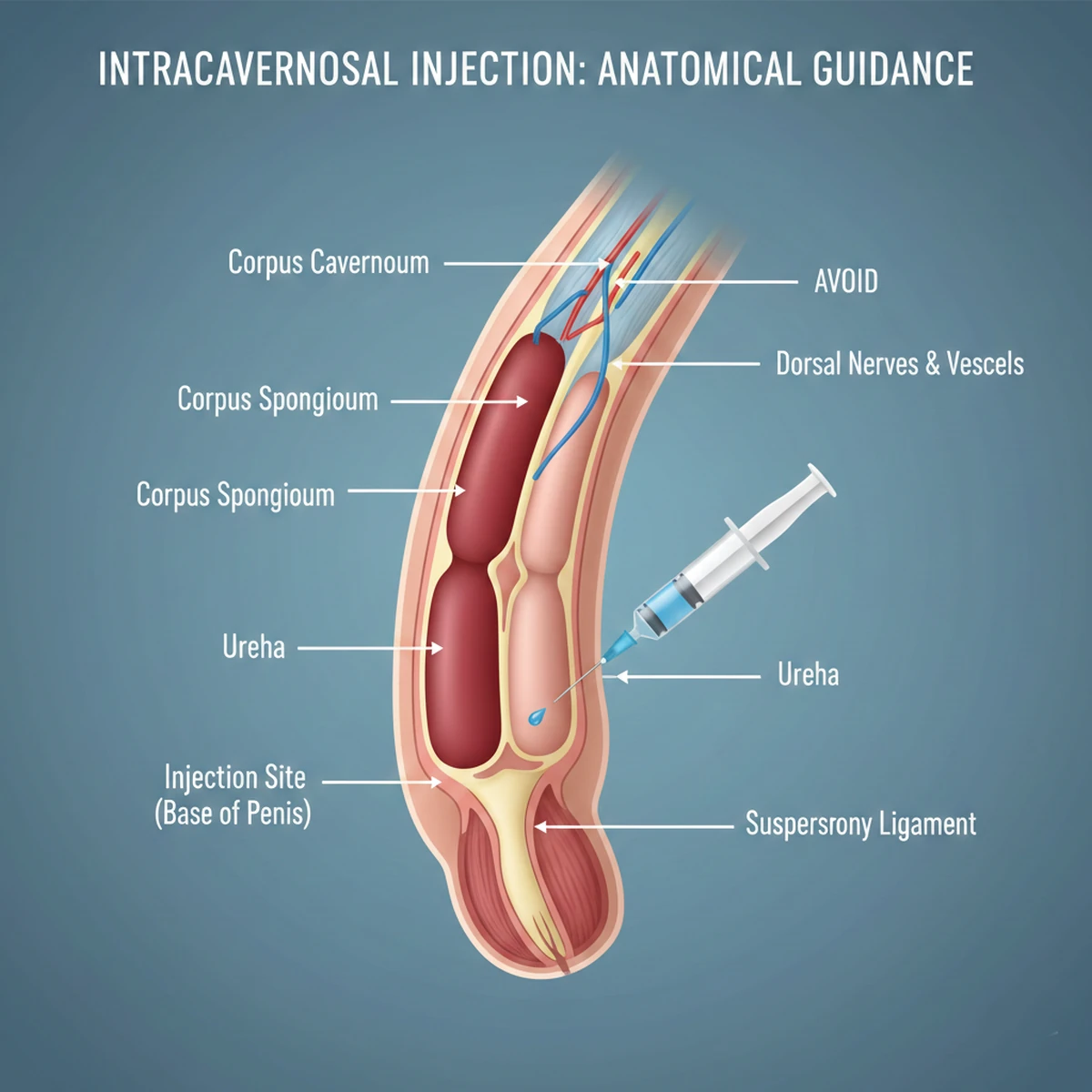
Targeted administration within the corpora cavernosa allows localized delivery of regenerative cellular components to areas of vascular and neurogenic compromise. This approach aims to optimize the penile microenvironment by supporting endothelial recovery and structural tissue integrity.
Intravenous Regenerative Cellular Therapy (Systemic Support)
Systemic endothelial repair concept image
Vascular inflammation modulation schematic
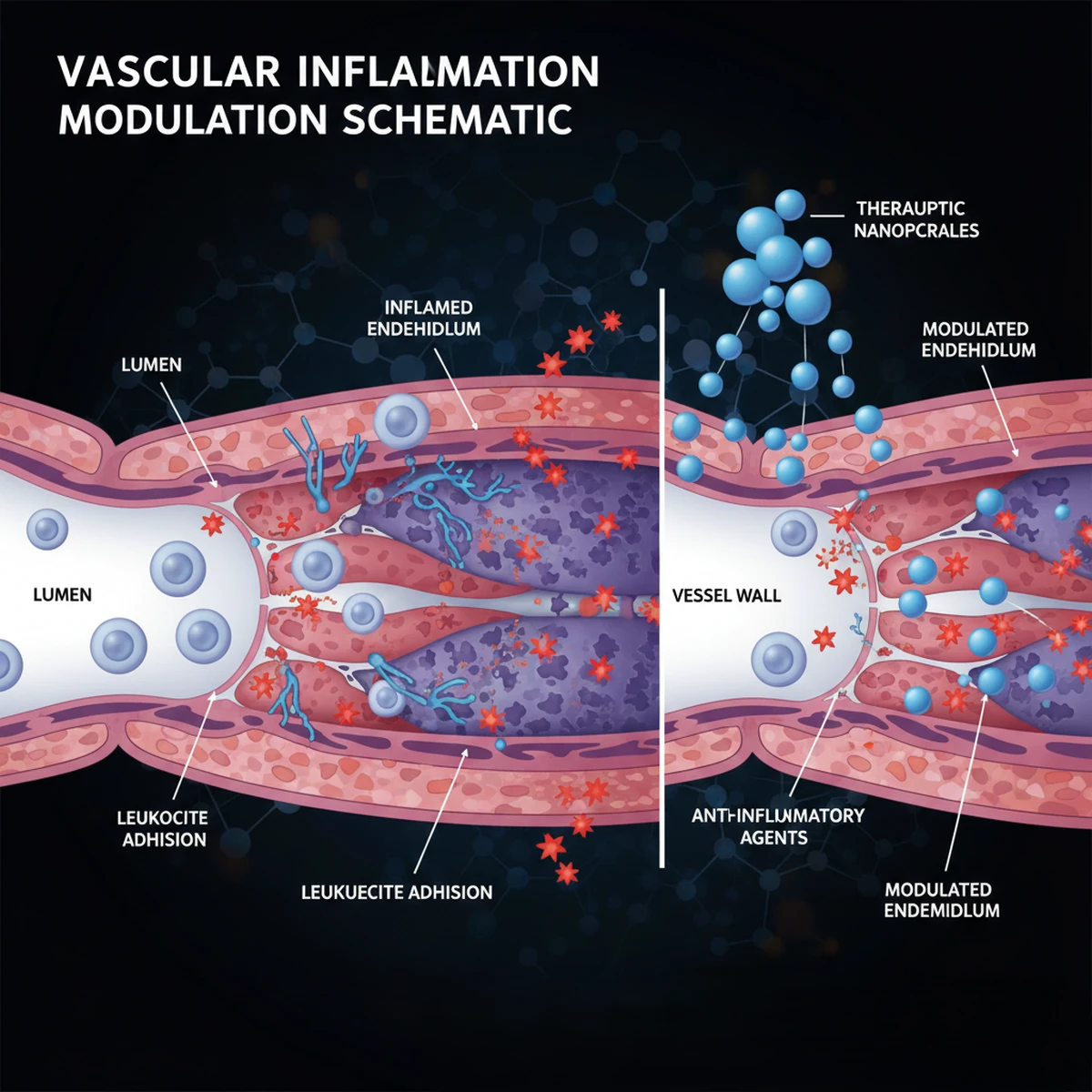
Intravenous delivery is considered in selected patients with systemic vascular dysfunction, metabolic syndrome, or diabetes-related endothelial impairment. The objective is broader vascular optimization and inflammatory modulation, which may indirectly support erectile function.
Exosome-Based Therapy (Localized & Intravenous Applications)
Exosome microscopy image
Extracellular vesicle signaling diagram
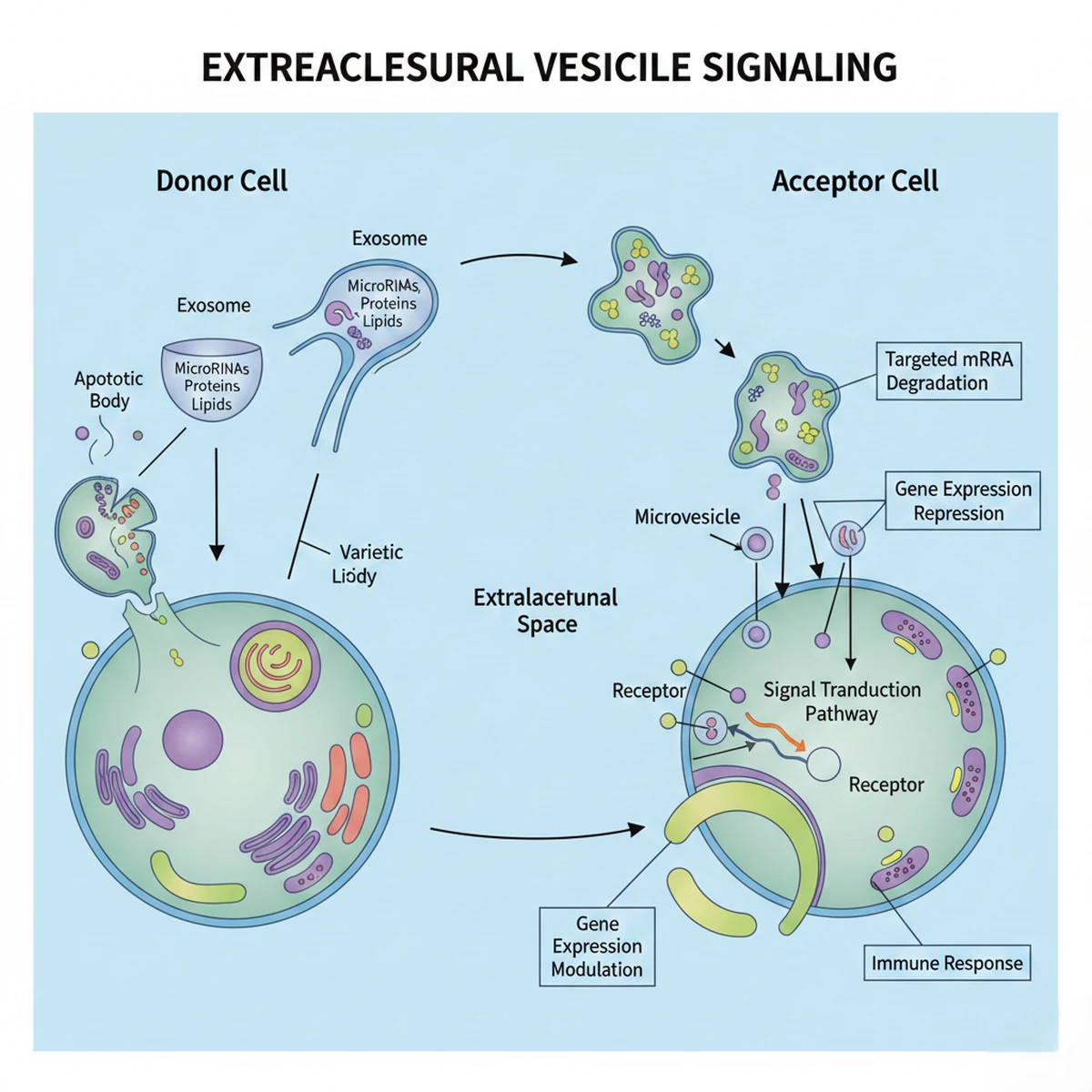
Cellular communication pathway illustration
Exosomes are extracellular vesicles involved in intercellular signaling. In regenerative research, they are investigated for their potential to:
- Support angiogenic signaling pathways
- Reduce pro-inflammatory mediators
- Enhance endothelial responsiveness
- Support neural microenvironment stability
Exosome therapy may be delivered locally (intracavernosal) to support penile tissue signaling or intravenously in selected cases to assist systemic vascular health.
Combination Regenerative Strategy
In selected patients, localized cellular regenerative therapy may be combined with exosome-based therapy to optimize paracrine signaling and tissue response. Systemic administration may be considered where metabolic or vascular contributors are identified.
Combination protocols are individualized based on vascular assessment, metabolic profile, erectile severity, and prior treatment response.

Adjunctive Non-Surgical Therapies
Additional therapies may include:
- Low-Intensity Shockwave Therapy (LISWT) to stimulate angiogenic pathways
- Platelet-Rich Plasma (PRP) to support localized growth factor release
Integration of therapies is based on clinical indication and medical necessity.
Comprehensive Clinical Evaluation
All patients undergo structured assessment including:
- Detailed sexual health history
- Erectile function scoring tools
- Cardiovascular risk evaluation
- Hormonal testing where indicated
- Diabetes and metabolic screening
- Lifestyle factor analysis
Treatment plans are personalized and aligned with current regulatory and safety standards.
Expected Outcomes
Some patients may experience gradual improvement in erectile rigidity, sustainability, and spontaneous erectile activity. Response depends on vascular integrity, systemic health, neural function, and adherence to medical guidance. No outcome can be guaranteed.
Frequently Asked Questions
Are regenerative cellular therapies safe?
When administered under licensed medical supervision with proper patient selection, these therapies are generally well tolerated. Individual risks are discussed during consultation.
What is the difference between localized and intravenous therapy?
Localized therapy targets penile tissue directly, while intravenous therapy focuses on systemic vascular and inflammatory optimization.
Can therapies be combined?
Yes, combination approaches may be considered when clinically justified.
How soon are results observed?
Regenerative therapies aim for gradual improvement over weeks to months.
Do you treat international patients?
Yes. Coordinated medical consultation and scheduling are available.

Self-Assessment Questionnaire for Erectile Dysfunction
Instructions: This self-assessment is intended for personal screening purposes only and does not replace a medical consultation. Answer each question honestly based on your experience over the past 6 months.
This questionnaire is a screening tool only and is not diagnostic. Information provided here is for educational purposes.