- Small Penis Treatment Dubai
- Longevity Health Check Dubai
- Male Genital Cosmetology Dubai
- Male Sexual Problems Treatment Dubai
- Prevention Health Check Dubai
- Premature Ejaculation Treatment in Dubai
- Erectile Dysfunction Treatment in Dubai
- Azoospermia (Zero Sperm Count) Treatment in Dubai
- Peyronie’s Disease Treatment in Dubai
- Reduced Penile Girth Treatment in Dubai
Premature Ejaculation Treatment in Dubai
Advanced premature ejaculation treatment in Dubai using cellular rejuvenation and exosome therapy. A discreet, non‑surgical regenerative approach.
Life’s journey is deeply personal, and so are the concerns we face along the way. At Lumora Wellness, led by the renowned Dr. Vasan, we recognize that addressing genital growth and development concerns goes beyond physical appearance—it’s about restoring confidence, comfort, and emotional well-being. Every patient has a story, and we are here to help write a new chapter filled with solutions, support, and renewed self-assurance.
Regenerative & Targeted Neuromodulation Approach
At Lumora Wellness, premature ejaculation (PME) is evaluated as a multifactorial neurophysiological condition. Our physician-led protocols integrate targeted neuromodulation and exosome-based regenerative therapy within a structured clinical framework.
This treatment approach is intended for carefully selected patients following comprehensive medical evaluation. All therapies are performed under licensed medical supervision in accordance with applicable UAE healthcare regulations.
Understanding Premature Ejaculation A Clinical Perspective
Premature ejaculation is characterized by reduced ejaculatory latency and diminished voluntary control, often associated with personal distress.
Contributing factors may include:
- Increased penile sensory nerve sensitivity
- Hyperactive ejaculatory reflex pathways
- Bulbospongiosus muscle overactivity
- Neurogenic inflammation Vascular instability
- Hormonal or metabolic influences
Conventional treatments such as SSRIs, topical anesthetics, and behavioral therapy may provide symptomatic benefit but may not address underlying neurophysiological contributors in all cases.
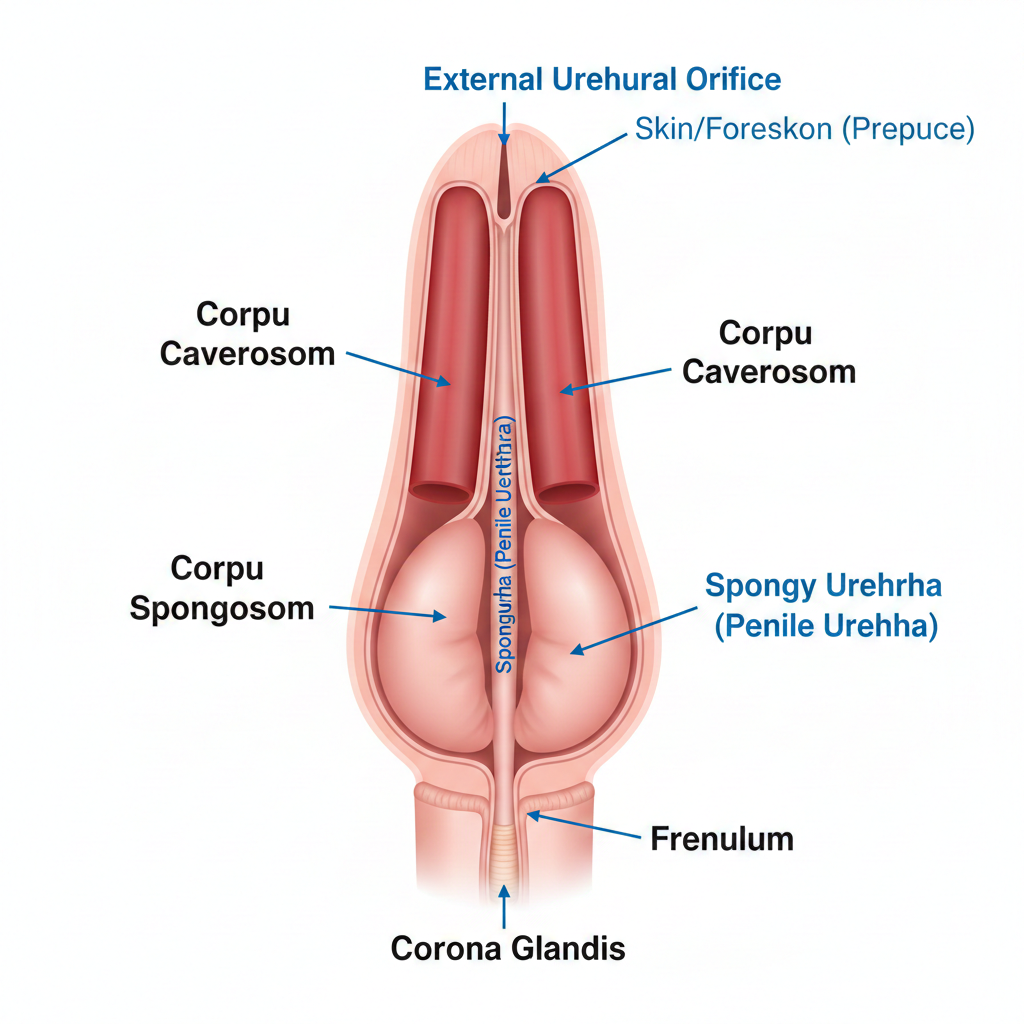
Glans Hypersensitivity (Anatomical Reference)
Penile glans anatomy diagram
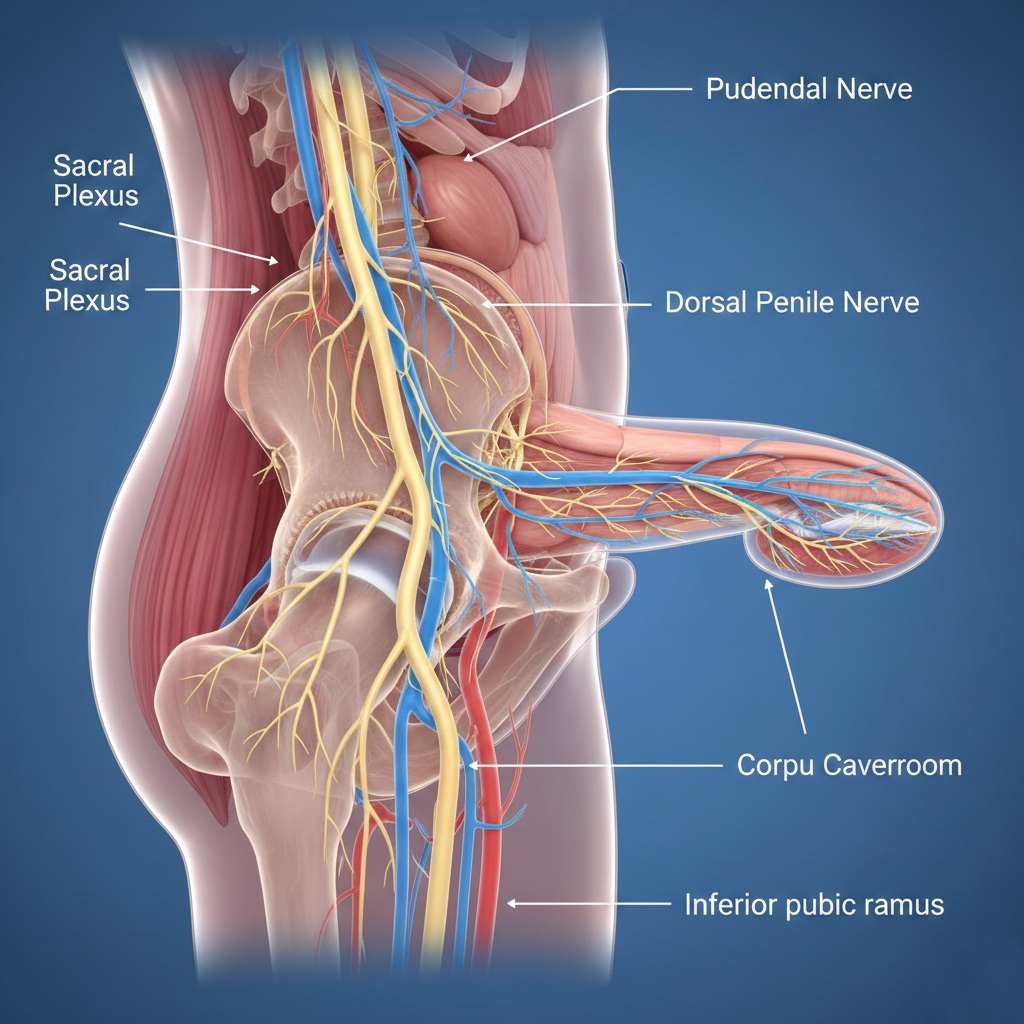
Dorsal penile nerve pathway
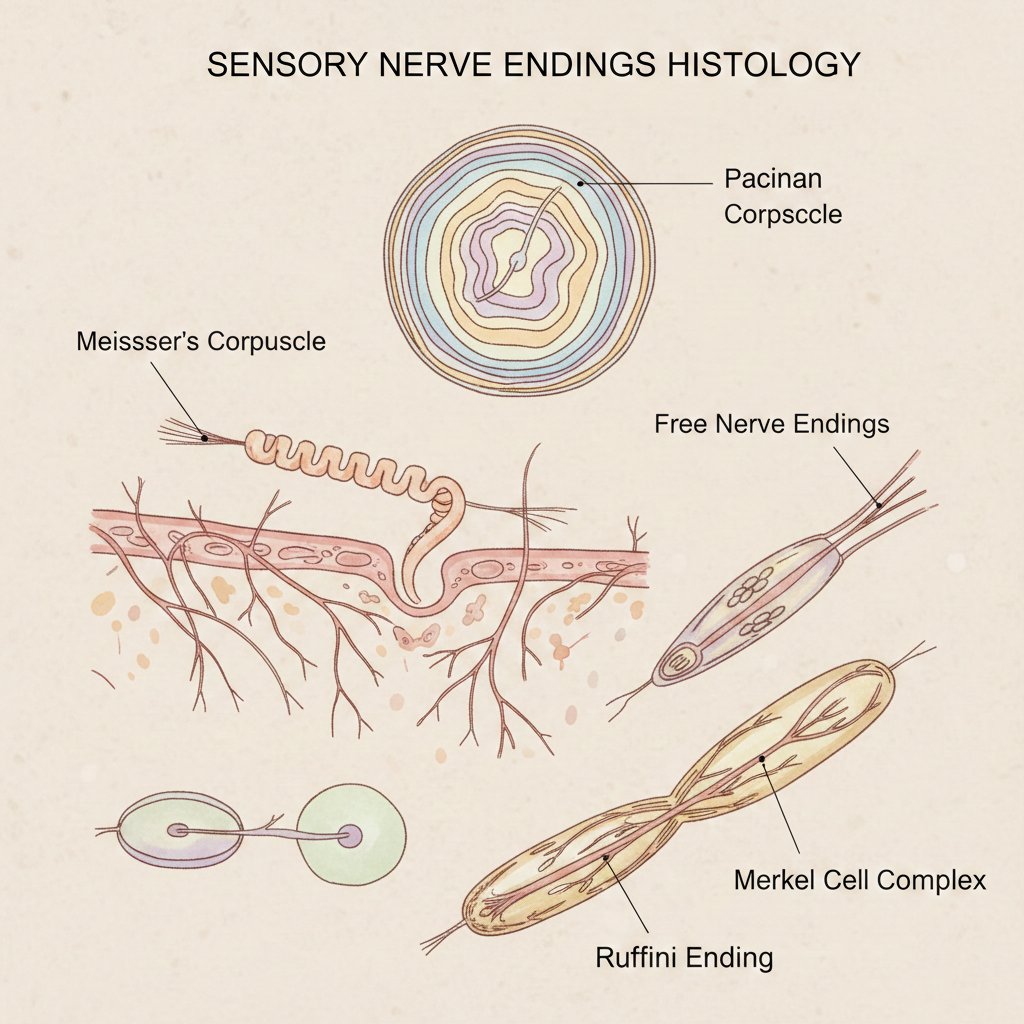
Sensory nerve endings histology
Male genital nerve supply overview
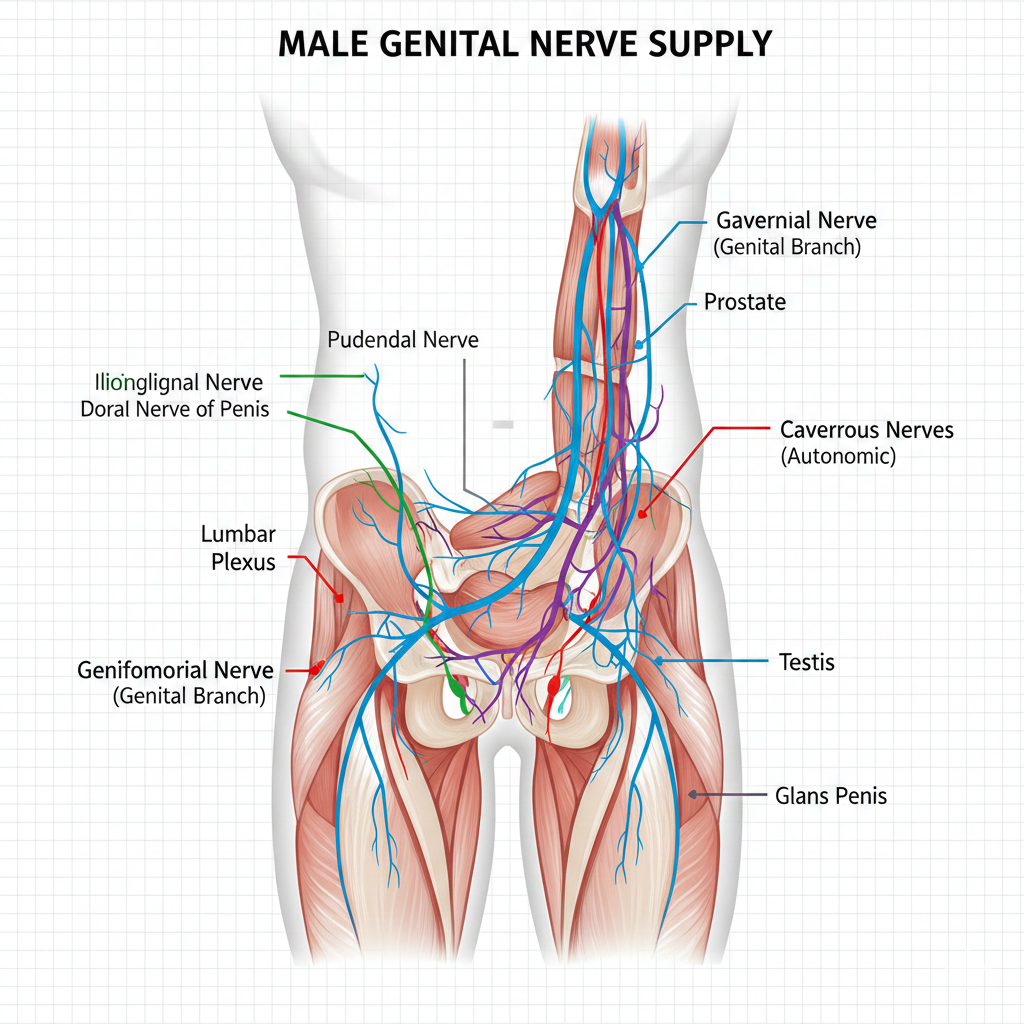
The glans penis contains a dense concentration of sensory receptors supplied primarily by the dorsal penile nerve. Reduced sensory thresholds or inflammatory signaling may contribute to heightened excitatory input and earlier reflex activation.
Bulbospongiosus Muscle & Ejaculatory Reflex Pathway
Bulbospongiosus muscle anatomy
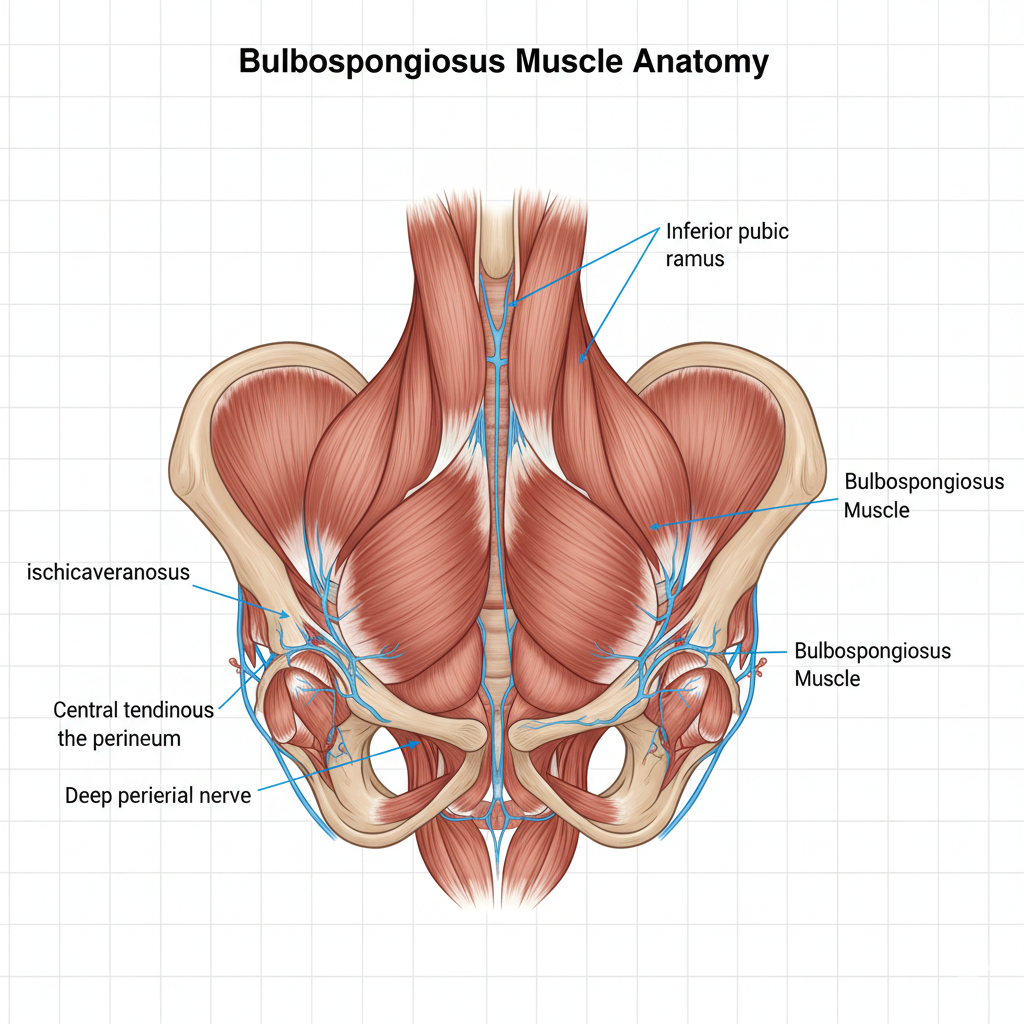
Male pelvic floor diagram
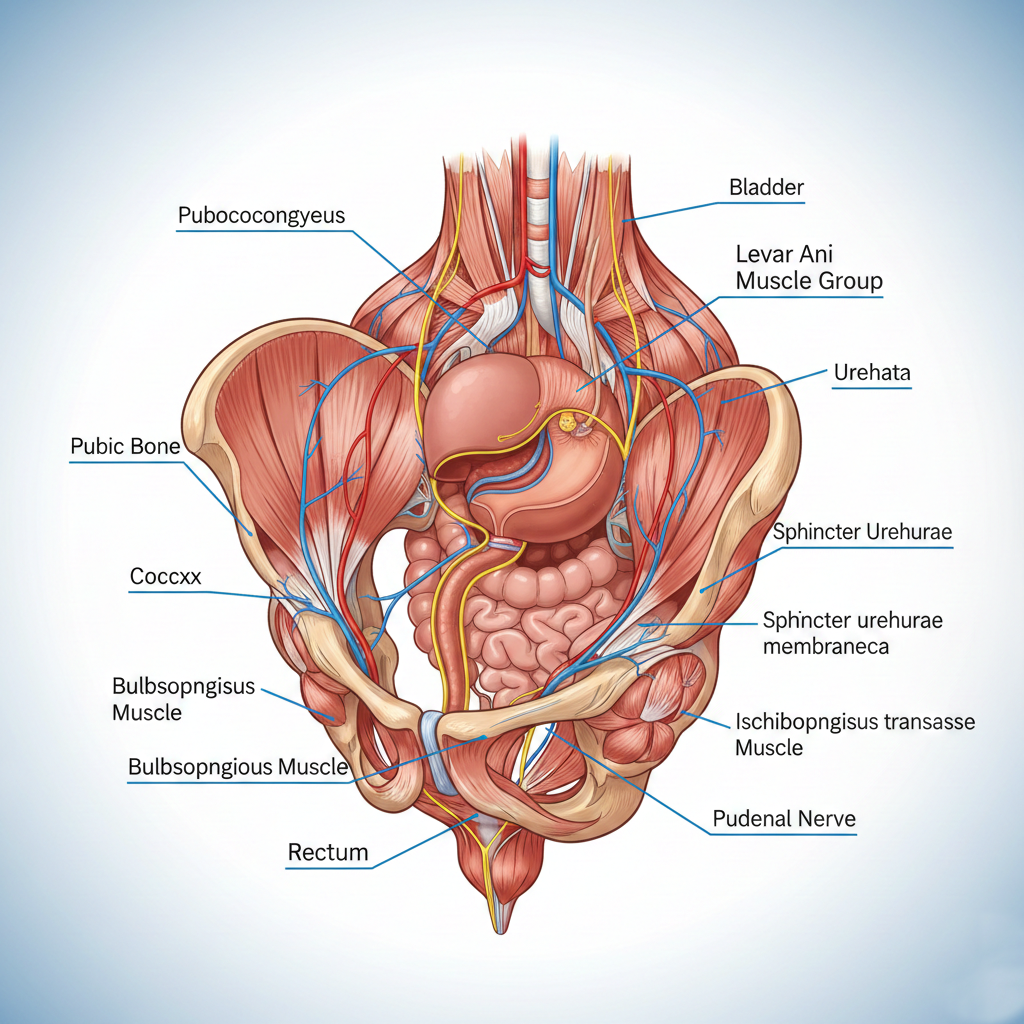
Ejaculatory reflex pathway

Perineal muscle anatomy
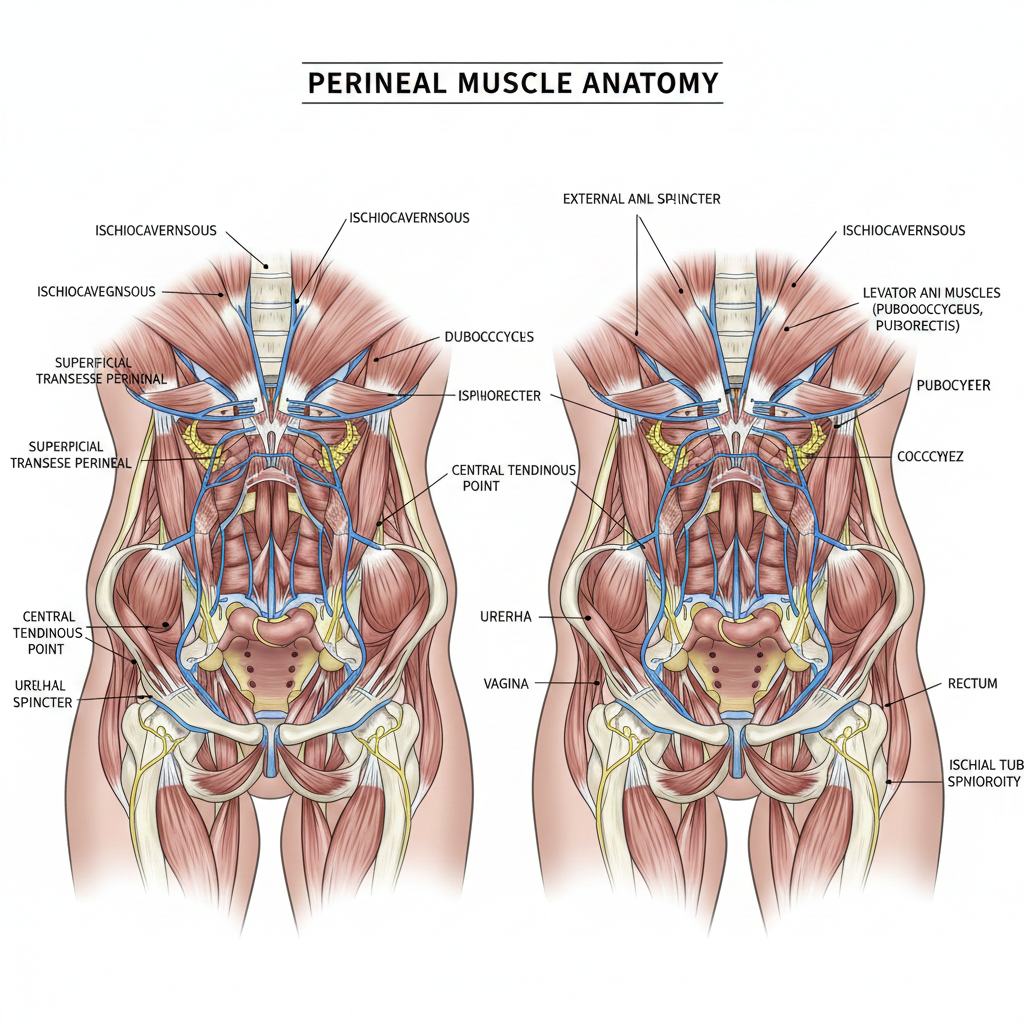
The bulbospongiosus muscle participates in rhythmic contractions during ejaculation. Increased neuromuscular excitability may reduce voluntary control.
Targeted Neuromodulation (Botulinum-Based Therapy)
Botulinum-based neuromodulation may be considered in carefully selected patients to modulate excessive neuromuscular activity.
Potential mechanisms include:
- Modulation of acetylcholine release
- Reduction of bulbospongiosus hypercontractility
- Support for improved reflex control
Suitability is determined through clinical evaluation. Outcomes vary, and effects may be temporary.

Exosome-Based Regenerative Therapy
Exosome electron microscopy image

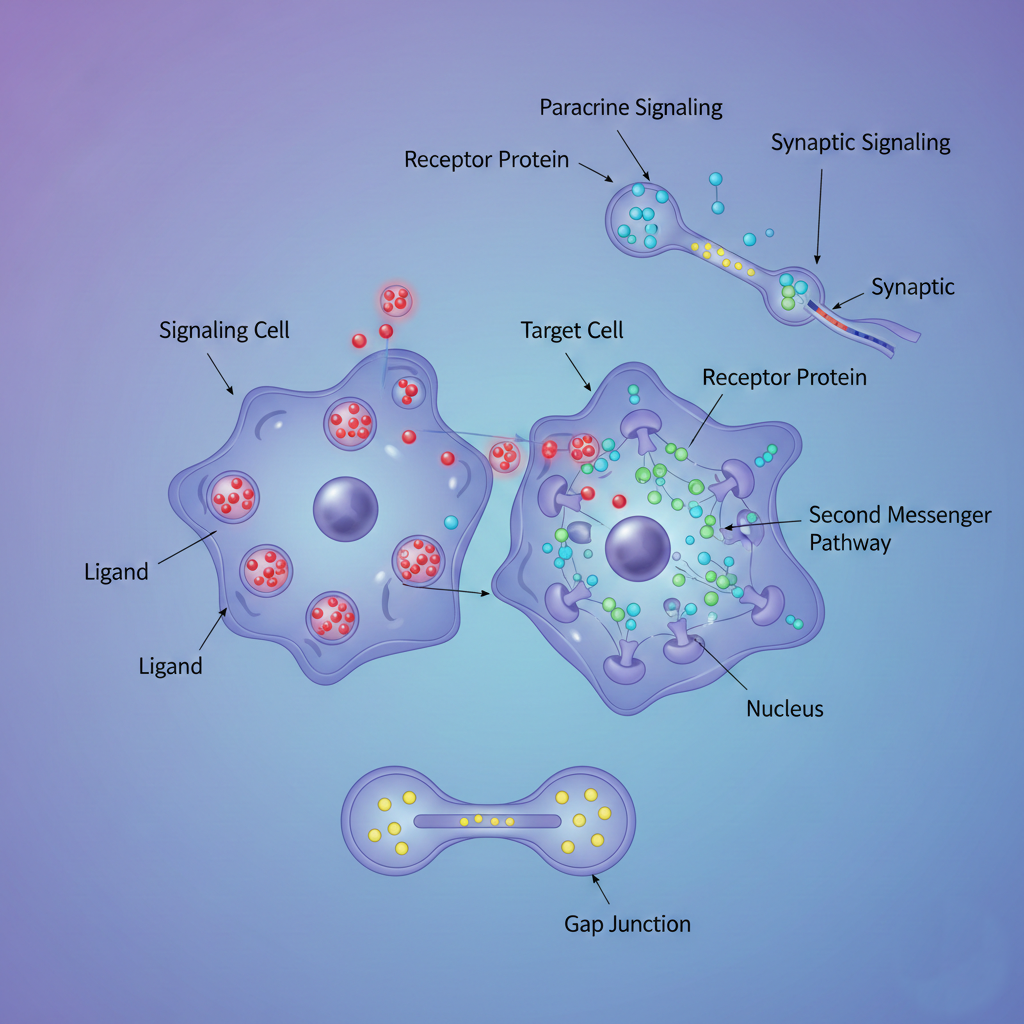
Extracellular vesicle signaling diagram
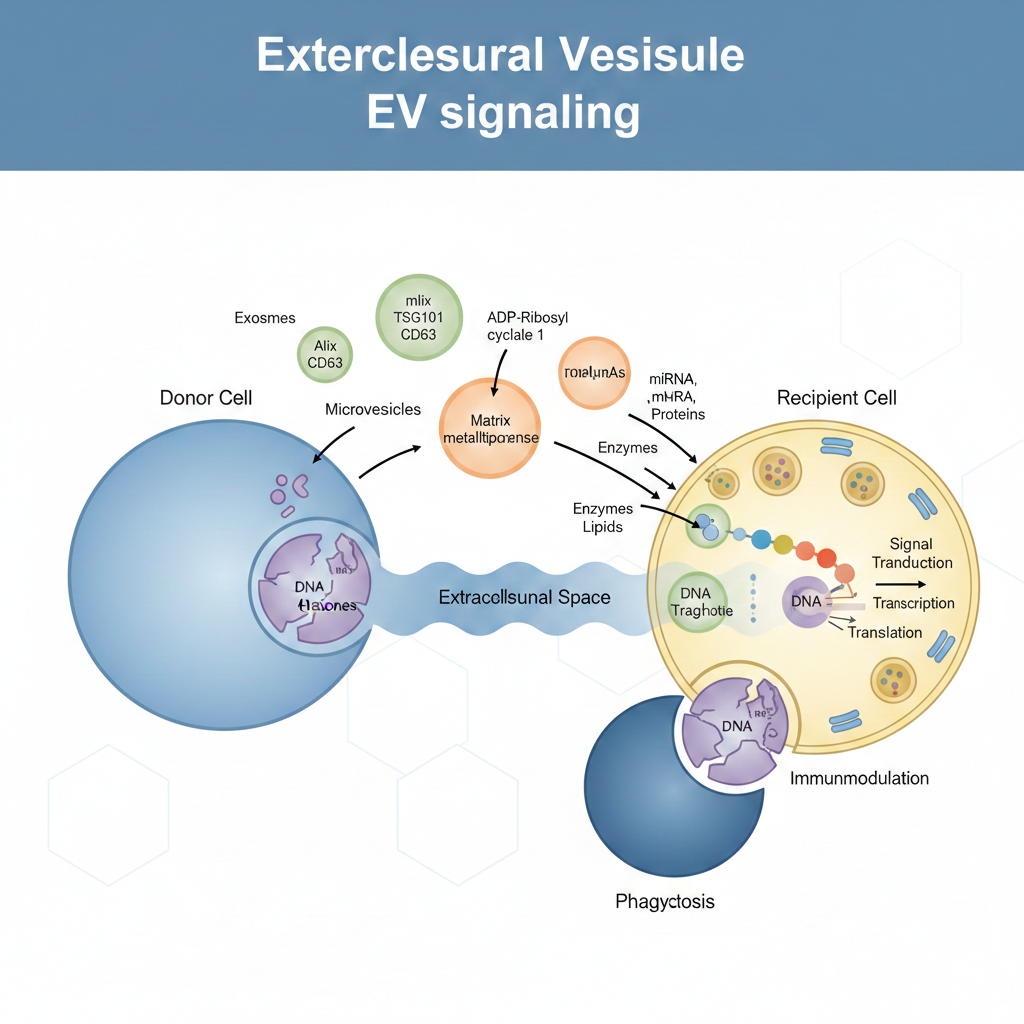
Cellular communication illustration
Nerve regeneration concept image
Exosomes are extracellular vesicles involved in intercellular communication. In regenerative medicine research, they are studied for their potential role in
- Modulating inflammatory pathways
- Supporting tissue signaling balance
- Influencing nerve repair mechanisms
- Promoting vascular endothelial function
Applications in sexual medicine are considered evolving and are offered under strict medical supervision following informed consent.
Why Destructive Procedures Are Not Preferred
Surgical nerve resection and cryotherapy aim to reduce sensation through tissue destruction. These approaches may carry risks including numbness, neuropathic discomfort, fibrosis, and irreversible changes.
Modern sexual medicine increasingly favors neuromodulation and regenerative approaches over permanent nerve damage where appropriate alternatives exist.
Clinical Evaluation Process
Each patient undergoes structured assessment including sexual health history, erectile function evaluation, hormonal and metabolic screening where indicated, and pelvic neuromuscular assessment. Treatment recommendations are individualized and based on medical necessity.
Expected Outcomes
Some patients may experience improvement in ejaculatory latency, reduced hypersensitivity, enhanced control, and improved confidence. Clinical response varies based on individual physiology and comorbidities. No outcome can be guaranteed.
Frequently Asked Questions
What is premature ejaculation (PME)?
Premature ejaculation is characterized by reduced ejaculatory latency, diminished voluntary control over ejaculation, and associated personal or relational distress.
What causes PME?
PME may involve multiple contributing factors including penile sensory hypersensitivity, exaggerated ejaculatory reflex pathways, pelvic floor muscle overactivity, neurogenic inflammation, vascular instability, hormonal imbalance, or psychological contributors.
Is PME purely psychological?
No. While psychological factors can contribute, many patients demonstrate measurable neurobiological and neuromuscular factors.
How is PME diagnosed?
Diagnosis is based on clinical history, assessment of ejaculatory latency, evaluation of erectile function, and identification of contributing medical or neurological factors.
Can PME occur later in life?
Yes. Acquired PME may develop after a period of normal function and may be associated with erectile dysfunction, prostate conditions, metabolic disorders, or stress.
What treatment options are available?
Options may include behavioral therapy, oral medications, topical agents, pelvic floor therapy, targeted neuromodulation, and regenerative therapies where clinically appropriate.
Are regenerative therapies guaranteed to work?
No medical treatment can guarantee results. Clinical response varies depending on individual physiology and contributing factors.
Is treatment safe?
All treatments should be performed under licensed medical supervision following appropriate clinical evaluation and informed consent.

Self-Assessment Questionnaire for Premature Ejaculation
Instructions: This self-assessment is intended for personal screening purposes only and does not replace a medical consultation. Answer each question honestly based on your experience over the past 6 months.
This questionnaire is a screening tool only and is not diagnostic. Information provided here is for educational purposes.